
A polio surveillance officer downloads data from vaccinators' phones at the end of the day's polio vaccination campaign in Jere, Nigeria, 2020. ©️ Andrew Esiebo/WHO
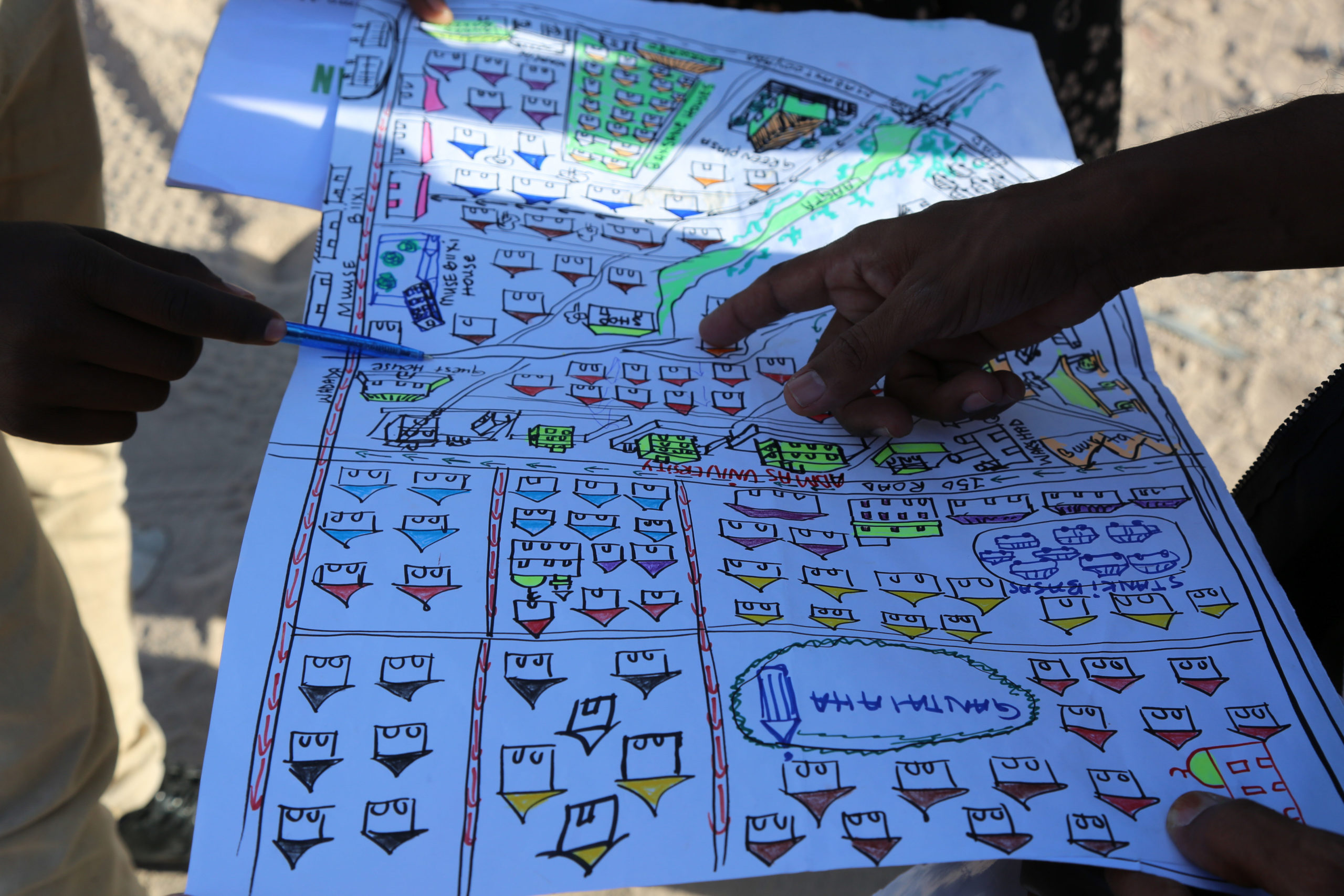
GIS applications are used alongside traditional maps, such as this one showing residential areas targeted for polio vaccination, Hargeisa, Nigeria, 2019. ©️ WHO

A vaccinator opens up the mobile technology AVADAR on their mobile phone, 2020. ©️ Andrew Esiebo/WHO

A WHO team trains community volunteers and health workers on the user of AVADAR in Gurai, South Sudan, 2019. © WHO/AFRO

Using e-SURV, conversations with health workers in the field are guided by a simple questionnaire, which improves the quality and consistency of data collection, 2019. © WHO/Darcy Levison

Dr Adele Daleke Lisi Aluma speaks to Robert about the symptoms of measles, polio, and other vaccine-preventable diseases. His answers are recorded using e-SURV, and transmitted to a central database. © WHO/Darcy Levison


Vaccinators in Juba prepare for a vaccination campaign during a national immunization day campaign targeting 3.7 million children in South Sudan, 2017. ©️ UNICEF